The title seems ordinary enough, but hidden in it's meaning is the life of the first woman ophthalmologist of color. One who broke through 'the glass ceiling' as early as 1974.
For those who speak of breaking through a glass ceiling for women.....you are a bit late ! Medicine however offers an undeniable metric for advancement, achievement and dedication. In other disciplines such as business financial measures, leadership ability or political persuasion are more amorphous measures for a 'glass ceiling.
Patricia Bath's career path runs very similar to
Ben Carson, MD (former Presidential candidate for President of the United States. She was born in poverty, and went to what some would call a second rate School of Medicine. That was the last step in 'second rate' institutions. From there she was accepted to a major world class ophthalmology training program, eventually earning faculty status.
For me as the average white male American I don't think I can fully appreciate her journey. With all the privilege of being white I still had challenges pursuing my education. The competition to become accepted to medical school is extremely high, the competition to be accepted into an ophthalmology training program is even more intense, and becoming the chair of an ophthalmology training program one of those 'never events' we speak of in complications of surgery.
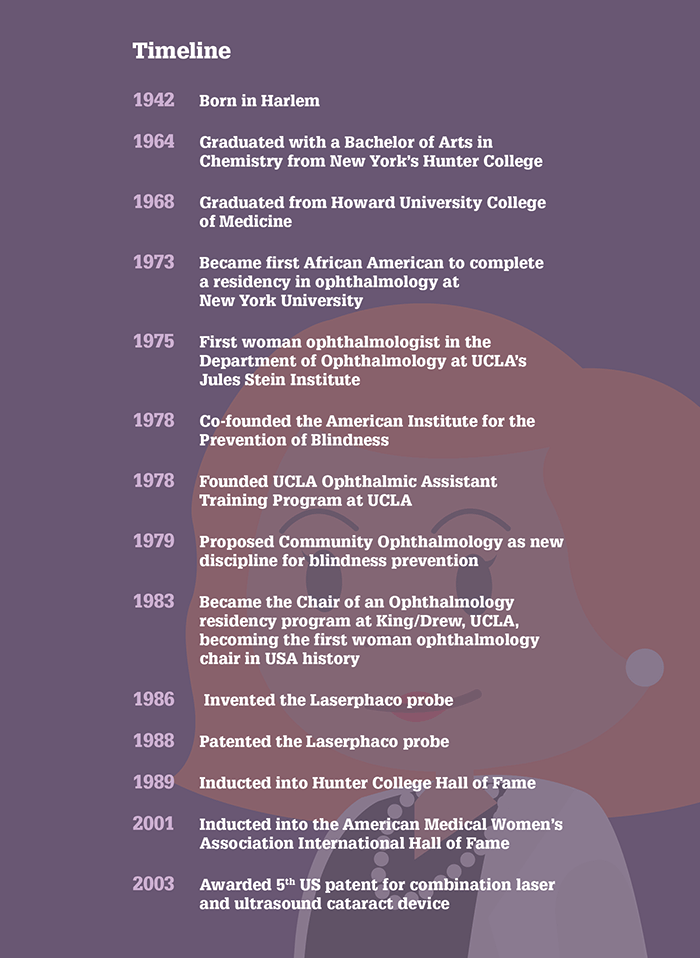
The graphic below succinctly maps her progress to recognition
The Career path of Patricia Bath M.D. F.A.A.O.
Her inspirational thoughts will fuel the desire of many more women and men of color.
When she chould not penetrate an impregnable barrier, she went around it, preferring to not waste energy and to pursue her own interest. All of which is evident from her outcome.
My favorite motivational saying is "Believe in one-self" Ask few for opinions (be sure who you ask in t he first place. Don't listen to negative answers. Remain committed to your goals. Find people who believe in you and will assist you, or at least not stand in your way.
I salute all the 'suffragettes who strive to improve humanity with their standards, goals.
This post gave me great pleasure, one of the most enjoyable as well as satisfying, to recognize a great physician (ophthalmologist) I have written (in my humble opinion)
Gary M. Levin M.D. F.A.A.O.
more.......
Lessons I’ve Learned








