The future for the Affordable Care Act may well live in the minds of the current generation of medical students and trainees and not the electorate or political party. In reality the future of medicine is in their destiny.
Journal of General Internal Medicine: March 10, 2015
BACKGROUND
It is not known whether medical students support the Affordable Care Act (ACA) or possess the knowledge or will to engage in its implementation as part of their professional obligations.
PARTICIPANTS
All 5,340 medical students enrolled at eight geographically diverse U.S. medical schools (overall response rate 52 % [2,761/5,340]).
CONCLUSIONS
The majority of students in our sample support the ACA. Support was highest among students who anticipate a medical specialty, self-identify as political moderates or liberals, and have an above-average knowledge score. Support of the ACA by future physicians suggests that they are willing to engage with health care reform measures that increase access to care.
KEY RESULTS
The majority of respondents indicated an understanding of (75.3 %) and support for (62.8 %) the ACA and a professional obligation to assist with its implementation (56.1 %). The mean knowledge score from nine knowledge-based questions was 6.9?±?1.3. Students anticipating a surgical specialty or procedural specialty compared to those anticipating a medical specialty were less likely to support the legislation (OR?=?0.6 [0.4-0.7], OR?=?0.4 [0.3-0.6], respectively), less likely to indicate a professional obligation to implement the ACA (OR?=?0.7 [0.6-0.9], OR?=?0.7 [0.5-0.96], respectively), and more likely to have negative expectations (OR?=?1.9 [1.5-2.6], OR?=?2.3 [1.6-3.5], respectively). Moderates, liberals, and those with an above-average knowledge score were more likely to indicate support for the ACA (OR?=?5.7 [4.1-7.9], OR?=?35.1 [25.4-48.5], OR?=?1.7 [1.4-2.1], respectively) and a professional obligation toward its implementation (OR?=?1.9 [1.4-2.5], OR?=?4.7 [3.6-6.0], OR?=?1.2 [1.02-1.5], respectively).
Author's Opinion
Judging from the survey result the majority of trainees support the ACA and will work with the new system. This is not surprising. Young physicians are altruistic and by and large are not driven by monetary aspects. of health care. Few are knowledgable about the inner workings of the payment system until they enter practice. It would be interesting to survery physicians in age groups centering around their length in practice. Perhaps the quote, "Old dogs do not learn new tricks" would be appropriate.
Tuesday, March 17, 2015
Monday, March 16, 2015
What Does a Technology Optimist Think about the Future of Health Care?
One of my favorite reads are articles by Robert Wachter M.D. His latest post on KevinMD yesterday speaks to the subject of technology and optimism for the future of health care. Wachter is enthusiastic about IT, but also tells precautionary thoughts. This post appears on KevinMD
A series of Wachter's articles appears here:
Andy McAfee is the associate director of the Center for Digital Business at MIT’s Sloan School of Management. He is also coauthor (with his MIT colleague Erik Brynjolfsson) of the 2014 book, The Second Machine Age: Work, Progress, and Prosperity in a Time of Brilliant Technologies, one of my favorite books on technology. While he sits squarely in the camp of “technology optimists,” he is thoughtful, appreciates the downsides of IT, and isn’t overawed by the hype. In the continuing series of interviews I conducted for my forthcoming book on health IT, The Digital Doctor: Hope, Hype, and Harm at the Dawn of Medicine’s Computer Age, I spoke to McAfee on August 13, 2014 in a restaurant in Cambridge, Massachusetts. I began by asking about some of the general lessons from today’s world of technology and business that have implications for health care.
Bob Wachter interviews Andy McAfee
A series of Wachter's articles appears here:
Andy McAfee is the associate director of the Center for Digital Business at MIT’s Sloan School of Management. He is also coauthor (with his MIT colleague Erik Brynjolfsson) of the 2014 book, The Second Machine Age: Work, Progress, and Prosperity in a Time of Brilliant Technologies, one of my favorite books on technology. While he sits squarely in the camp of “technology optimists,” he is thoughtful, appreciates the downsides of IT, and isn’t overawed by the hype. In the continuing series of interviews I conducted for my forthcoming book on health IT, The Digital Doctor: Hope, Hype, and Harm at the Dawn of Medicine’s Computer Age, I spoke to McAfee on August 13, 2014 in a restaurant in Cambridge, Massachusetts. I began by asking about some of the general lessons from today’s world of technology and business that have implications for health care.
Bob Wachter interviews Andy McAfee
McAfee: Our devices are going to continue to amaze us. My iPhone — it’s a supercomputer by the standards of 20 or 30 years ago. Right now, hundreds of millions of people carry a device that is about this powerful. Wait a little while. That number will become billions. And those devices will spit out ridiculous amounts of data of all forms, so this big data world that we’re already in – that’s going to accelerate.
Since data is the lifeblood of science, we’re going to get a lot smarter about some pretty fundamental things, whether it’s genomics or self-diagnosis or how errors happen. Then, because we’re putting all this power into the hands of so many people all around the world, it seems certain that the scale, pace, and scope of innovation are going to increase.
So I’m truly optimistic for the medium- to long-term. But the short-term is going to be a really interesting, really rocky time.
RW: When you say medium- to long-term, how many years before we get to this wonderful place?
AM: Don’t hold me to it. But within a decade.
RW: We always like to think we’re special in medicine. We’re so different. It’s so complicated. Do you see any fundamental differences between health care and other industries that will shape our technology path?
AM: There are two main things that might retard progress in medicine. The first is health care’s payment system, particularly how messed up it is trying to match who benefits versus who pays. The other thing is the culture of medicine. I understand that it’s changing, but there’s still this idea that “how dare you second-guess me, I’m the doctor.”
RW: But we can’t be alone in that. I’m sure many industries have their stars — supported by their guilds — who think, “We’re at the top of the heap, with high income and stature. We’re going to fight this technology thing since it could erode our franchise.”
AM: Sure, but in the rest of the world eroding the franchise is what it’s all about. It’s Schumpeterian creative destruction [the theory advanced by Austrian economist Joseph Schumpeter — it is, in essence, economic Darwinism, and forms the core of today’s popular notion of “disruptive innovation”], so if you’re behind the times and I’m not, I’m going to come along and displace you, and the market will speak to that.
I asked McAfee about some of the negative consequences of technology I explore in my book, particularly the issues of human “deskilling” and the changes in relationships – for example, the demise of radiology rounds because we don’t have to go to the radiology department to see our films anymore.
AM: Technology always changes social relationships, and it often leads to the erosion of some skills. The example I always use is that I can’t use a slide rule. I was never trained to do that. Whereas engineers at MIT a generation before me were really, really good with their slide rules.
RW: Are there other industries in which people are now smart enough to say, “This is likely to be the impact of this new technology on social relationships, and here is how we should mitigate the harm”? Or do they just implement, see what happens, and then ask, “What have we lost and how do we deal with that?”
AM: Much more the latter. I haven’t seen a good playbook for “here’s what is going to happen when you put this technology and, therefore, do these three things in advance.” It’s much more that you have some thoughtful people saying, “Wait a minute. We used to do X and we kind of liked that and now we do less of X, so it’s turned into Y. We need to put some Z in place.”
RW: Does Z tend to be some high-tech relationship connector?
AM: In some cases, yeah. But there’s the story about the call center that was unhappy about some aspects of its social relationships. They just moved the break room and the break times so that people literally would just come and hang out a lot more. That made people a lot happier, and it made the outcomes better. Sometimes the fix has a tech component, and sometimes it doesn’t.
As in many of my interviews, we turned to the question of whether computers would ultimately replace humans in medicine. I described a few situations in which physicians use “the eyeball test” — their intuition, drawn from subtle cues that are not (currently) captured in the data — to make a clinical judgment.
AM: The great [human] diagnosticians are amazing. But we still pat ourselves on the back about them far too much and we ignore or downplay or we think that we are exceptions to the really well identified problems of this particular computer [McAfee points to his brain]. The biases, the inconsistencies, the fact that if I’m going through a divorce, or I have a hangover, or I’ve got a sick kid, so my wiring is all messed up.
Have you ever met anyone who thought they had below average intuition or was a below average judge of people, or they were below average in recognizing sick patients? You’ll never meet that person. We have a serious problem with overconfidence in our own computers.
While severing the human link would be a deeply bad idea, much of what we currently think of as this uniquely human thing is, in fact, a data problem. The technology field called machine learning — and a special branch of it called deep learning — is just blowing the doors off the competition. We’re getting weirdly good at it very, very quickly.
In addition, my geekiest colleagues would say, “OK. You think you’ve started data collection for this situation? You haven’t even begun. Why don’t we put a high def camera on the patient? For every encounter, we can assess skin tone. We can code for their body language. Let’s put a microphone in there. We’ll code for their speech tones.”
And then we’ll see which patterns are associated with schizophrenia, diabetes, Alzheimer’s. We’ll do pattern-matching on a scale that humans can never, never equal. In other words, our IT systems don’t care if the guy went to the intensive care unit two hours later or was diagnosed with Parkinson’s 20 years later. Just give us the data.
RW: How much of health care will be in the hands of patients and their technology? How much are they going to be monitoring themselves, independent of doctors or hospitals or other traditional health care organizations?
AM: It’s hard to imagine how that won’t come to pass. They’ll monitor the hell out of themselves. They’re going to have peer communities that they probably rely on a lot and they’re going to have algorithms guiding their treatment or their path.
I turned to the question of diagnosis, and particularly the issue of probabilistic thinking. The context was the 40-year history of predictions that computers would ultimately replace the diagnostic work of clinicians, predictions that, by and large, did not pan out.
RW: In medicine, there’s no unambiguously correct answer a lot of the times. It’s a probabilistic notion. I call something “lung cancer” or “pneumonia” when the probability is above a certain threshold, and I say I’ve “ruled out” a diagnosis when the probability is below a certain threshold. Setting these thresholds depends on the context, the patient’s risk factors, and the patient’s preferences. I also need to know how accurate the tests are, how expensive they are, and how risky they are. And often the best test is time – you decide to reassure the patient, not do anything, and then see how things go.
AM: Yeah. That complicates the work of the engineers. Not immeasurably, but it does make it a lot more complicated. But I imagine that there are a bunch of really smart geeks at IBM’s Watson eagerly taking notes as guys like you describe these kinds of situations. In their head they’re thinking, “How do I model all of that?”
Bob Wachter is a professor of medicine, University of California, San Francisco. He coined the term “hospitalist” and is one of the nation’s leading experts in health care quality and patient safety. He is author of Understanding Patient Safety, Second Edition and The Digital Doctor: Hope, Hype, and Harm at the Dawn of Medicine’s Digital Age. He blogs at Wachter’s World, where this article originally appeared.
Despite the challenge of affordability and access the future does look optimistic.
Bonus Material on Social Media
A Surgery Standard Under Fire
What she wanted, the patient told the geriatricians evaluating her, was to be able to return to her condominium in Boston. She had long lived there on her own, lifting weights to keep fit and doing her own grocery shopping, until a heart condition worsened and she could barely manage the stairs.

So at 94, she consented to valve replacement surgery at a Boston medical center. “She never wanted to go to a nursing home,” said Dr. Perla Macip, one of the patient’s geriatricians. “That was her worst fear.”
Dr. Macip presented the case on Saturday to a meeting of the American Academy of Hospice and Palliative Medicine. The presentation’s dispiriting title: “The 30-Day Mortality Rule in Surgery: Does This Number Prolong Unnecessary Suffering in Vulnerable Elderly Patients?”
Like Dr. Macip, a growing number of physicians and researchers have grown critical of 30-day mortality as a measure of surgical success. That seemingly innocuous metric, they argue, may actually undermine appropriate care, especially for older adults.
The experience of Dr. Macip’s patient — whom she calls Ms. S. — shows why.
Ms. S. sustained cardiopulmonary arrest during the operation and needed resuscitation. A series of complications followed: irregular heartbeat, fluid in her lungs, kidney damage, pneumonia. She had a stroke and moved in and out of the intensive care unit, off and on a ventilator.
After two weeks, “she was depressed and stopped eating,” Dr. Macip said. The geriatricians recommended a “goals of care” discussion to clarify whether Ms. S., who remained mentally clear, wanted to continue such aggressive treatment.
But “the surgeons were optimistic that she would recover” and declined, Dr. Macip said.
Thirty-day mortality serves as a traditional yardstick for surgical quality. Several states, including Massachusetts, require public reporting of 30-day mortality after cardiac procedures. Medicare has also begun to use certain risk-adjusted 30-day mortality measures, like deaths after pneumonia and heart attacks, to penalize hospitals with poor performance and reward those with better outcomes.
However laudable the intent, reliance on 30-day mortality as a surgical report card has also generated growing controversy. Some experts believe pressures for superior 30-day statistics can cause unacknowledged harm, discouraging surgery for patients who could benefit and sentencing others to long stays in I.C.U.s and nursing homes.
Saturday, March 14, 2015
How Mayo's "Dr. Google" Deal Disrupts Medicine
“Dr. Google” has joined the Mayo Clinic, quietly signaling a powerful disruption for all of medicine.

Back in 1997 I wrote: “The information age is to medicine as the Protestant Reformation was to the Catholic Church.” The Church didn’t disappear when information once held tightly by the priesthood became widely available, but religion changed forever.
In that context, Mayo’s agreement to produce clinical summaries under its name for common Google medical searches is like a medieval pope happily handing out Bible translations. The mission of the most-used search engine on the planet is to make the world’s information “universally accessible and useful.” Mayo, in contrast, has for decades been a global symbol of doctor-knows-best. Recommending a Google search “as the first stop for those needing health information,” in the words of a Mayo physician executive, represents a true paradigm change.
About 5 million patients nationwide currently have electronic access to open notes. Boston’s Beth Israel Deaconess Medical Center and a few other institutions are letting patients make additions and corrections to what they call “OurNotes.” Not surprisingly, many doctors remain mortified by this medical sacrilege.
Patients are being invited to read their health record in "OurNotes" an adaptation of Open Notes
Gamification in Health Care Is Booming, but Is it Effective?


CUSTOM MOD DESKTOP

The report includes comments from:

SONY PLAYSTATION VITA

And even your smart devices

Monday, March 9, 2015
Hospital Rating Websites Vary Widely in Rankings, Study Finds
Ranking hospitals and providers is a complex procedure with serious pitfalls.
Four popular hospital rating websites vary widely about which facilities are the best and which are the worst, according to a study published on Monday in Health Affairs, Modern Healthcare reports (Rice, Modern Healthcare, 3/2).
Study Details
The researchers evaluated four rating sites that rank or grade hospitals across the country:



Findings
The researchers found that no hospital earned top ratings from all of the sites. Out of 844 hospitals that received a high rating from one site, just 10% earned top marks from another site. Meanwhile, 27 hospitals that received top ratings from one site received low marks from another.
The researchers noted that the variation in definitions of quality could confuse consumers, who increasingly are comparison shopping for medical services. In addition, the researchers said the different definitions could complicate hospitals' efforts to focus improvements.
Reaction
UCLA Health System Chief Medical Officer and Chief Quality Officer Robert Cherry said, "Unfortunately, we can attest as an institution that has come out on both sides of these 'report cards' that there is a lack of clarity, consistency and understanding between the various methodologies and in some cases [this] may be misleading the public" (Beck, Wall Street Journal, 3/2).
The ratings services said that their systems serve different purposes that consumers understand. "They're not measuring the same thing," Healthgrades Chief Strategy Officer Evan Marks said (New York Times, 3/2).
For example, Leapfrog uses a letter grade to reflect how well a hospital keeps patients from "preventable harm and medical errors," while Healthgrades compiles a list of top hospitals using mortality and complication rate data.
Doris Peter, director of Consumer Reports' health-ratings center, said the findings are "not a surprise to us -- we're rating different aspects of hospital quality," adding, "we are all hampered by needing better data" (Wall Street Journal, 3/2).
The researchers said the ratings are useful, but study author Matthew Austin, an assistant professor at the Johns Hopkins University School of Medicine, emphasized that consumers needed to understand the ratings systems' different focuses and their limitations. He added it is necessary for the systems to increase efforts to communicate their ratings' goals. Austin also said that the challenge for a ratings system is finding a grade or category that is easily understood but still represents an institution's nuances (New York Times, 3/2).
Thursday, March 5, 2015
How Will Congress Respond to Supreme Court Ruling on Obamacare Subsidies?
A potential crisis is looming with an upcoming Supreme Court Ruling on the Affordable Care Act.
Once again the poorly constructed Affordable Care Act is creating chaos and confusion alike for providers and patients.
Why we are still talking about Obamacare.
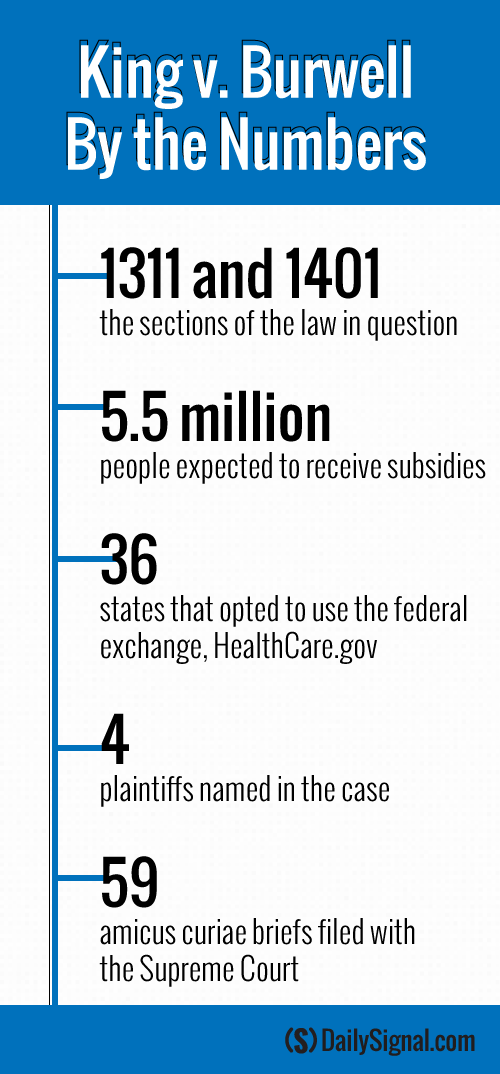
 At 10 a.m. tomorrow, the nine U.S. Supreme Court justices will take their places on the bench in the marble temple to hear oral arguments in the highly anticipated case King v. Burwell.
At 10 a.m. tomorrow, the nine U.S. Supreme Court justices will take their places on the bench in the marble temple to hear oral arguments in the highly anticipated case King v. Burwell.
Once again the poorly constructed Affordable Care Act is creating chaos and confusion alike for providers and patients.
Why we are still talking about Obamacare.
Millions of Americans will have to wait several months before the high court decides the future of the subsidies available under the Affordable Care Act, but eyes are already looking from the Supreme Court to Capitol Hill for how lawmakers plan on responding to a ruling.
Republicans in the House and Senate are working to finalize legislation that would help Americans transition from the current system should the Supreme Court rule against the Obama administration.
“[The] question is: Then what?” Republican Reps. John Kline, Paul Ryan and Fred Upton wrote in an op-ed for The Wall Street Journal last night. “What about the people who will lose their subsidies—and possibly their coverage? No family should pay for this administration’s overreach.”
Though nothing has been finalized, the lawmakers are pushing for patient-centered reforms that transfer control of the insurance market from the federal government back to states.
Though nothing has been finalized, the lawmakers are pushing for patient-centered reforms that transfer control of the insurance market from the federal government back to states.
History of the Case
King v. Burwell addresses whether states operating on the federal exchange are eligible for subsidies under the Affordable Care Act.
As it’s written, the law granted subsidies to customers who purchase coverage “through an exchange established by the state.” It also granted the Department of Health and Human Services the authority to create a federally-run exchange, HealthCare.gov, for states that choose not to run their own.
>>> Commentary: Q&A: What Is at Stake in the King v. Burwell Case?
Following the states’ decisions, the IRS issued a ruling that extended the tax credits to include states using HealthCare.gov.
The tax agency’s decision raised red flags for opponents of the Affordable Care Act who argue the IRS violated the law. However, the government has said that in order for the law’s insurance reforms to be successful, nationwide subsidies are needed.
Now, the high court will decide whether the 36 states using HealthCare.gov are permitted to offer tax credits to their residents.
House Republicans Present Their Plan
The Supreme Court isn’t expected to announce a ruling on King v. Burwell until June. However, experts are looking to lawmakers on Capitol Hill to ready a transition plan should the court rule against the Obama administration.
If that happens, health policy experts estimate that approximately 5.5 million Americans could lose their subsidies and see the price of their premiums increase drastically, as the subsidies help keep the costs of health plans down.
“If the court rules against the administration, as any fair reading of the law would demand, millions of individuals and families will hit a major road block: They’ll be stuck with health insurance designed by Washington, D.C., they can’t afford,” Republicans Kline, Ryan and Upton wrote.
Kline, Ryan and Upton are chairman of the House Education and Workforce, Ways and Means, and Energy and Commerce Committees, respectively.
To mitigate the fallout from the increased cost in premiums and lost subsidies, the trio of lawmakers revealed their “off-ramp from Obamacare”—the result of a working group made of House Republicans that designed a proposal for those potentially affected by the Supreme Court’s decision.
The plan is made up of two parts: The first authorizes states to opt out of the Affordable Care Act’s coverage requirements and the employer and individual mandates. The second part of the plan would secure “advanceable” and “refundable” tax credits for states affected by the Supreme Court’s decision.
“So here’s the bottom line: Under Obamacare, government controls your choices,” the Republicans wrote. “Under our proposal, you will. You’ll get to pick a plan that works for you.”
Senate Counterparts Offer Their Ideas
Echoing the actions of their House counterparts, a trio of Republican Senate leaders penned their own op-ed in the Washington Post to discuss their answer to King v. Burwell.
Sens. Lamar Alexander, Orrin Hatch and John Barrasso, heads of the Senate Health, Education, Labor and Pensions Committee, Finance Committee and Republican Policy Committee, respectively, outlined their plan to help Americans at risk of losing their subsidies.
“When the court rules in King v. Burwell, we anticipate that it will hold the administration to the laws Congress passed, rather than the laws the administration wishes Congress had passed, and prohibit subsidies in states that opted not to set up their own exchanges, as the language of the law clearly states,” they wrote.
The senators’ plan includes providing financial assistance to affected Americans that would allow them to keep their original coverage for a “transitional period.”
“People do not deserve further disruption from this law,” they said.
Additionally, their plan would give power back to states and allow them to design their own health care system.
“[A ruling against the administration] would also give Congress an opportunity—to stop Obamacare’s damage and create a pathway to reforms that move our health care system in the direction of freedom, choice and lower cost,” Alexander, Hatch and Barrasso said.
Experts’ Ideas
The congressional Republicans are in lockstep with aspects of policy proposals offered by conservative experts in response to the Supreme Court’s decision.
Nina Owcharenko and Ed Haislmaier, health policy experts at The Heritage Foundation, outlined their answer to King v. Burwell in a paper released last week.
“Congress and the states should therefore seize the opportunity and clear the way for patient-centered, market-based reforms to take root in the states,” the pair wrote.
The experts encouraged Congress to exempt those in affected states from the Affordable Care Act’s insurance regulations, as well as the individual and employer mandates. Additionally, Owcharenko and Haislmaier advised lawmakers to pass pre-emptive legislation shifting plans from being federally regulated to state-regulated.
However, the experts advised Congress to abandon the “complex and costly subsidies of the ACA,” as they are accompanied by rules, restrictions and penalties.
“The design of the subsidies creates major financial incentive for millions of Americans to shift to plans that qualify for the new subsidies,” they wrote.
The Obama Administration’s Plan
White House officials contend that both those for and against the Affordable Care Act agreed that it was generally understood that those who joined the federal exchange were eligible for the law’s subsidies. And both the president and Health and Human Services Secretary Sylvia Mathews Burwell believe the Supreme Court will uphold the law as it’s currently interpreted.
However, neither the president nor Burwell said they have a contingency plan for if the high court rules the other way.
“We know of no administrative actions that could, and therefore we have no plans that would, undo the massive damage to our health care system that would be caused by an adverse decision,” Burwell wrote in a letter to Republicans last week.
In an interview with Reuters, the president echoed Burwell’s statements.
“If they rule against us, we’ll have to take a look at what our options are,” Obama said. “But I’m not going to anticipate that. I’m not going to anticipate bad law.”
>>> Commentary: What Alexander Hamilton Would Say About King v. Burwell
Content attributed to the Daily Signal
Subscribe to:
Comments (Atom)
(Castlemen'' Disease)
Castleman disease is a group of rare disorders that involves lymph nodes that get bigger, called enlarged lymph nodes, and a wide range of s...

-
David’s Health Tech Newsletter: No. 62 – “Companies Disrupting Healthcare In 2015” via reddit.com The 21st Century has shown rapid develo...
-
(click for locations) Or is it Doctor Google ? Either you are a lover or a hater of all things Google. Google however has some thing...
-
At the intersection of health, health care, and policy.At the intersection of health, health care, and policy. A Four Years Into A C...
