Sunday's Health Train is making many stops on our journey...Consider these a new bullet train.
INCREDIBLE: A team of renegade doctors has exposed 18 alternative cancer treatments the mainstream tried to bury. They defy Big Pharma’s narrative and put survival back in the hands of the people. These methods are backed by science, many are low-cost or even free, and they’re delivering results that terrify the medical cartels.
Cancer is fed by lies, and the hospitals profit from misery. But these 18 methods prove there’s another way.
Ketogenic Diet – Starves cancer cells of glucose, cutting off their lifeline. Patients report slowed growth, even remission.
Exercise – Activates immunity, destroys cancer cells, reduces inflammation, and restores strength.
Stress Reduction, Sleep, Sunshine – Stress fuels tumors. Deep sleep repairs, while sunlight boosts Vitamin D and immunity.
Vitamin D3 – Low levels linked to higher cancer risk. Supplementing blocks cell proliferation.
Propranolol – A heart drug that starves cancer cells of stress hormones they need to spread.
Melatonin – Not just for sleep. Shields healthy cells, boosts immunity, and kills cancer cells.
Metformin – A diabetes drug cutting off cancer’s sugar supply. Proven to slow tumor growth.
Curcumin/Nanocurcumin – Anti-inflammatory, anti-tumor, triggers cancer cell death.
Ivermectin – Demonized during COVID, now revealed to sabotage cancer cell survival.
Mebendazole/Fenbendazole/Albendazole – Anti-parasitic drugs that stop cancer cells from dividing.
Green Tea – EGCG compound blocks tumor growth and blood vessel formation.
Omega-3 Fatty Acids – Reduce inflammation, slash risks of breast, prostate, and colon cancers.
Berberine – Ancient plant compound, regulates sugar and kills cancer cells.
Statins – Cholesterol drugs with hidden anti-cancer effects.
Viagra, Cialis, Levitra – Blood flow enhancers making chemo deadlier against tumors.
Disulfiram – Alcoholism drug that destroys cancer’s survival pathways.
Ashwagandha – Ancient herb, cuts stress, boosts immunity, halts tumor growth.
Itraconazole – Antifungal that blocks cancer’s growth channels.
This isn’t speculation. These treatments are backed by research but buried to protect billion-dollar chemotherapy industries. The truth is being censored because a healed population doesn’t make money.
There are however no clinical rtrials and little interest by Pharma, because they are all readily available and not covered by health insurance
The world is waking up. The Deep State’s medical machine is cracking. These 18 therapies are weapons of survival, tools of liberation. Cancer was never just a disease—it was a business model. That business model is collapsing.
Take this seriously. Share this with those who need it most. This knowledge is power. This knowledge is life.
The American Medical Association represents less than 15% of practicing physicians.
It controls the CPT code system that governs how every physician in America gets paid.
It receives licensing fees from that system regardless of AMA membership.
It lobbies on behalf of positions most physicians actively oppose. It endorsed policies that accelerated consolidation, employment, and the commoditization of physician labor for decades.
The AMA doesn’t represent physicians.
It licenses the billing infrastructure they’re forced to use.
It controls the CPT code system that governs how every physician in America gets paid.
It receives licensing fees from that system regardless of AMA membership.
It lobbies on behalf of positions most physicians actively oppose. It endorsed policies that accelerated consolidation, employment, and the commoditization of physician labor for decades.
These are different things.
The conflation is not accidental.
“Is an AI doctor better than no doctor at all?”
It's the wrong question for a very real problem - healthcare access and capacity. That said, I think the medical training model gives us the best analogy for answering it anyway. Lemme explain...

Think about what a medical student does well:
→ More time and patience to take complete medical histories
→ Can look up, synthesize, and summarize diagnosis and treatment plans
→ Often takes more comprehensive notes than their attending
But medical students lack the clinical judgment to connect the dots in every situation. They can't yet navigate the interprofessional complexity of real care. They struggle with the non-clinical dimensions of medicine that no textbook covers.
So what do we do? We let med students work autonomously on those tasks where they're spikey-good, but attendings maintain oversight and own ultimate responsibility for the patient.
We are at a similar stage with AI in healthcare right now.
AI is spikey. Incredibly good at specific tasks - in fact, better than physicians at some of them. It can research and synthesize clinical information faster than any human doctor alive.
Sure, AI hallucinates - but it never gets tired. Let's not forget: physicians make errors too, and more so when they're tired.
Over time, healthcare AI will get less spikey - not because the spikes disappear, but because it will grow more of them. It will reach "doctor-level" autonomy across more and more activities. At some point, for a large range of tasks, it may feel almost resident-like... fairly darn autonomous.
But full medical licensure for AI? Unlikely. Not because it won't have comparable technical skill, but because most people still want humans orchestrating AI, not the other way around (for safety, ethical, and just plain human reasons).
So in reality, the most likely path isn't a fully licensed AI doctor. It's a human physician orchestrating a team of highly skilled AI resident agents - each spikey-good at specific high-value tasks. The human owns liability and gains the leverage to care for more patients with the same time and effort.
Some patients - low-risk, routine - may interact primarily with AI (and this is already happening!). The doctor becomes the manager: watching for deviations, running quality checks, talking directly to the patients they're worried about.
The right question was never "is an AI doctor better than no doctor?"
Because the honest answer is: “yes, but only for specific tasks... which means it's not really a full AI doctor at all.”
So the better question is: how can AI give every clinician more leverage to care for more patients - without burning out the humans who hold the whole system together?
July 1,1966, I remember the date well.
It was the first day of my medical internship at Boston University Medical Center and the very same day the first Medicare patients were admitted to the hospital.
I thought I knew my path. Two years of training, my second at the Boston City Hospital, then off to the U.S. Navy as a Lieutenant under the Berry Plan. What I did not know was that I would have a front row seat to a 60-year “project” that would fundamentally transform American medicine.
The “Medical Arms Race”
It began with reimbursement.
When Medicare launched, hospitals were reimbursed based on their reported costs, including capital investments in equipment and facilities, plus a margin. Financial risk for adopting new technology was minimal. The predictable result was a “medical arms race.” Hospitals competed by acquiring advanced imaging, surgical suites, and specialized capabilities.
At the same time, the payment structure rewarded procedures more generously than cognitive care. Surgical and interventional services generated higher reimbursement than time spent diagnosing complex, chronic illness.
The incentives were clear.
Over time, those incentives shaped career decisions.
When I graduated from medical school, there were nineteen specialty boards and no subspecialty boards. Today, physicians choose from more than two dozen specialty boards and nearly ninety subspecialties.
That expansion did not happen by accident. It followed the money.
Current workforce trends tell the rest of the story. The majority of graduating internal medicine residents, 70% now choose hospitalist roles, 20% pursue subspecialty training and a small minority, 10% enter traditional outpatient general internal medicine.
We should not be surprised that it is difficult to find a primary care physician.
From the beginning, Medicare’s payment structure favored acute intervention over longitudinal cognitive care. Sixty years later, we have built a system that reflects those priorities, technologically advanced, procedurally sophisticated, and economically aligned toward intervention.
Preventive and diagnostic medicine, the slow work of thinking, listening, and managing complexity over time remains comparatively undervalued.
We did not lose our primary care foundation by accident.
We redesigned the incentives.
If we were building Medicare today, would we structure it the same way?
A Single 20g Dose of Creatine Increases Cognitive Processing Speed by 24.5% Within 3.5 Hours
A double-blind, placebo-controlled trial found that creatine rapidly enhanced brain bioenergetics and improved cognitive performance during sleep deprivation, with effects lasting up to nine hours.
Creatine has long been regarded as just a muscle supplement — something for the gym that requires weeks of “loading” to saturate muscle stores. A recent randomized trial overturns that assumption.
In a randomized, double-blind, placebo-controlled crossover trial published in Scientific Reports, researchers gave healthy young adults a single high oral dose of creatine monohydrate (0.35 g/kg — roughly 20 grams for most adults) during 21 hours of sleep deprivation. They then tracked both cognitive performance and real-time brain energy metabolism using advanced MR spectroscopy.
The results were not subtle. At the first post-dose assessment — approximately 3.5 hours after ingestion — participants demonstrated a 24.5% improvement in numeric processing speed (p = 0.0003). When data were pooled across all three overnight assessments (0 a.m., 2 a.m., 4 a.m.), language processing speed improved by 29.1% — the largest cognitive gain observed in the trial. And the effect didn’t fade quickly. Improvements in processing speed and task performance persisted across the next two measurement points — extending roughly nine hours after ingestion.
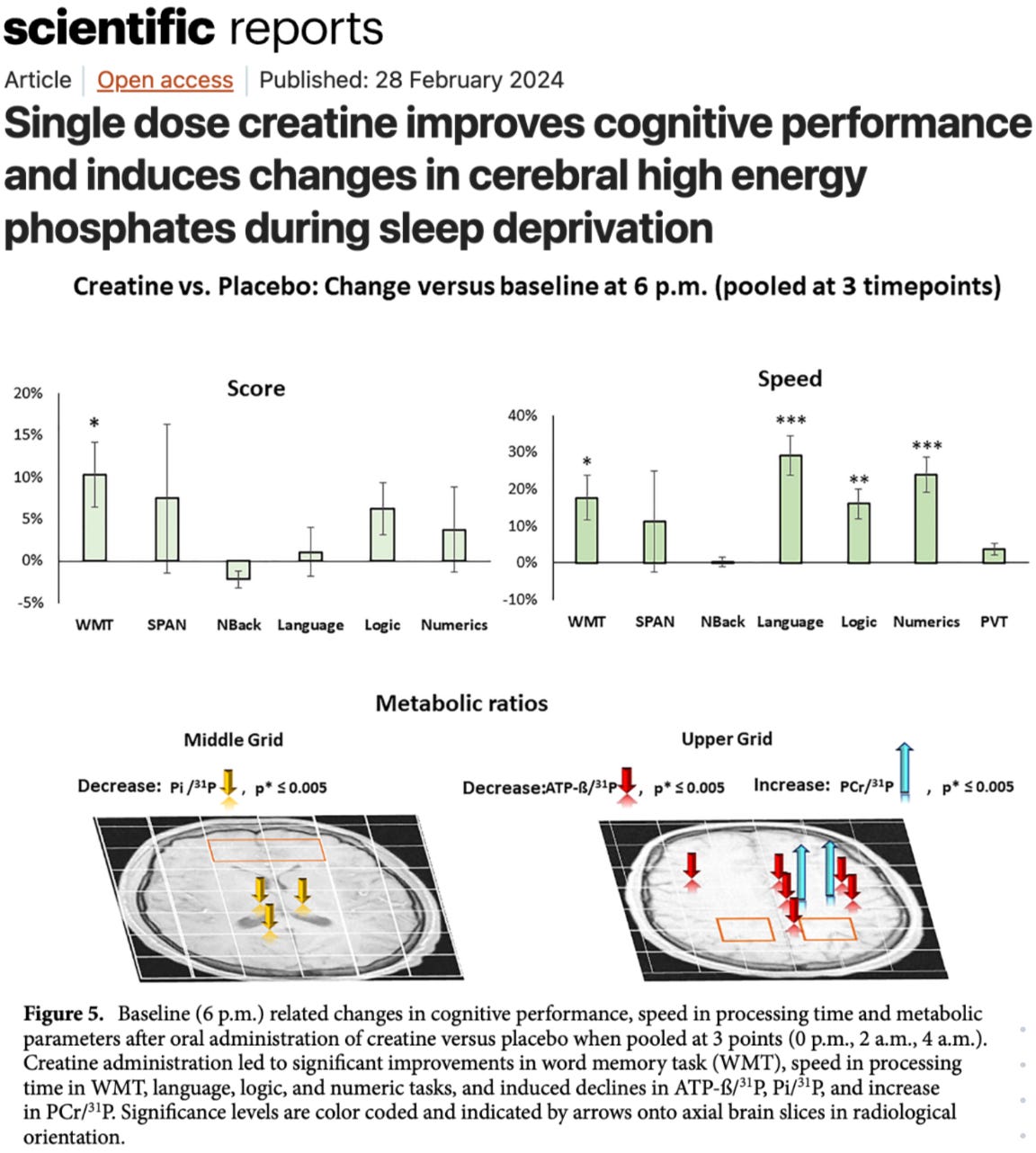
Just as important, the cognitive findings were mirrored by measurable metabolic shifts inside the brain. Creatine increased cerebral total creatine levels, prevented the typical sleep deprivation–induced drop in the PCr/Pi ratio (a marker of cellular energy stress), stabilized brain pH, and reduced subjective fatigue compared to placebo. In other words, this wasn’t just a behavioral effect — spectroscopy confirmed that high-energy phosphate metabolism itself was altered. The brain’s ATP buffering system appeared more resilient under stress.
In conclusion, a single ~20g dose of creatine rapidly enhanced brain bioenergetics and significantly improved cognitive performance during sleep deprivation, with effects sustained for up to nine hours.
******************************************************************


UnitedHealthcare, the largest Medicare Advantage provider in the United States, is implementing a new policy on May 1, 2026, that will require patients to receive a primary care provider (PCP) referral before seeing a cardiologist. This affects all patients enrolled in the insurer’s HMO and HMO-point of service (POS) Medicare Advantage plans.
The policy, which also covers cardiothoracic surgeons, vascular surgeons and several other specialties, officially went into place on Jan. 1. However, UnitedHealthcare announced at the time it would not start denying claims due to a lack of a referral until May 1. Existing referral policies in California, Nevada and Texas mean that PCP referrals have already been required in those states for all of 2026.
There are several exceptions to this new rule, including cardiac rehabilitation, physical therapy, dialysis and various emergency room/urgent care services. Medical imaging provided by a radiologist is another key exception.
“The referral requirement for specialist visits reflects the core design of HMO plans, which emphasize primary care‑led coordination,” a UnitedHealthcare representative told Cardiovascular Business. “Stronger PCP engagement can support earlier diagnosis, better chronic condition management, and more proactive care—ultimately contributing to improved health outcomes.”
The representative also emphasized that these referrals are effective as soon as they are submitted by the PCP.
Industry reactions to the new policy
There is a fear among many specialists that this added step will result in elderly patients missing out on care altogether. Securing an approval can be confusing for some patients, for instance, especially if they previously did not need a PCP referral to see a specific specialist.
There are also concerns about asking PCPs to take on additional work at a time when burnout is already high and physician shortages are already a significant problem throughout the United States.
Amit J. Shanker, MD, chair of the Heart Rhythm Society (HRS) Health Policy Committee and a Heart Rhythm Advocates board member, pointed to this policy is part of an ongoing issue with Medicare Advantage plans.
“There is a growing trend of hospitals and health systems terminating contracts with Medicare Advantage due to persistent prior authorization denials and delayed reimbursement,” he told Cardiovascular Business. “Over the past three years, approximately 90 health systems have severed ties with some or all Medicare Advantage plans. When hospitals drop plans, patients may face restricted physician access or higher out-of-pocket costs. This recent additional provision (effective May 1) by UnitedHealthcare further increases the barrier to cardiology access for patients.”
Meanwhile, Wendell Potter, a former health insurance executive who became a whistleblower and now advocates for policy reform, wrote about this update at length online. He said requiring these PCP referrals could save UnitedHealthcare “millions, if not billions of dollars” by reducing specialist visits. He also noted that the insurance juggernaut has “doubled down” on its efforts to shed high-cost patients in the wake of the 2024 murder of CEO Brian Thompson, a moment some analysts predicted might result in “kinder, gentler” policies.
Click here for additional information about the referral requirements for UnitedHealthcare’s Medicare Advantage HMO and HMO-POS plans.
CVS bars transparency
This was on X from Insurance Oligopoly.
The amendment now classifies MAC lists, reimbursement rates, and pricing terms as “Confidential Caremark Information.” It also states that providers cannot disclose, publish, distribute, or share this information without CVS Caremark’s permission.
The Consolidated Appropriations Act (CAA) specifically addressed gag clauses that restrict transparency around healthcare pricing and contract terms.
Yet we continue to see language that appears designed to limit visibility into how drugs are priced and reimbursed.
If employers are fiduciaries under ERISA, how are they supposed to ensure prudent oversight when critical pricing information is treated as confidential? Transparency in healthcare cannot exist without seeing the actual data.
When will we ENFORCE laws, words passed to act like you worked for the American people means NOTHING! Enforce the laws in place!!!



No comments:
Post a Comment