Once again the poorly constructed Affordable Care Act is creating chaos and confusion alike for providers and patients.
Why we are still talking about Obamacare.

Millions of Americans will have to wait several months before the high court decides the future of the subsidies available under the Affordable Care Act, but eyes are already looking from the Supreme Court to Capitol Hill for how lawmakers plan on responding to a ruling.
Republicans in the House and Senate are working to finalize legislation that would help Americans transition from the current system should the Supreme Court rule against the Obama administration.
“[The] question is: Then what?” Republican Reps. John Kline, Paul Ryan and Fred Upton wrote in an op-ed for The Wall Street Journal last night. “What about the people who will lose their subsidies—and possibly their coverage? No family should pay for this administration’s overreach.”
Though nothing has been finalized, the lawmakers are pushing for patient-centered reforms that transfer control of the insurance market from the federal government back to states.
Though nothing has been finalized, the lawmakers are pushing for patient-centered reforms that transfer control of the insurance market from the federal government back to states.
History of the Case
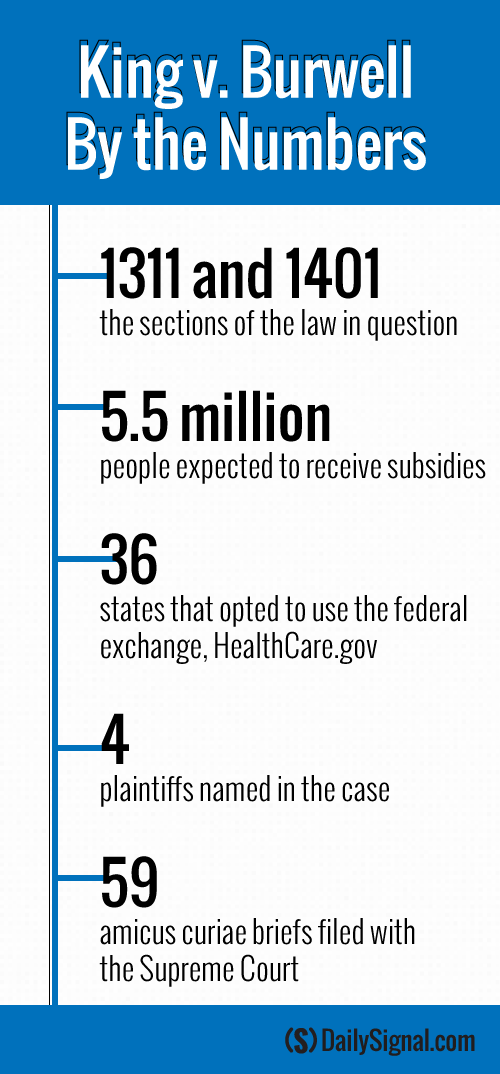
King v. Burwell addresses whether states operating on the federal exchange are eligible for subsidies under the Affordable Care Act.
As it’s written, the law granted subsidies to customers who purchase coverage “through an exchange established by the state.” It also granted the Department of Health and Human Services the authority to create a federally-run exchange, HealthCare.gov, for states that choose not to run their own.
>>> Commentary: Q&A: What Is at Stake in the King v. Burwell Case?
Following the states’ decisions, the IRS issued a ruling that extended the tax credits to include states using HealthCare.gov.
The tax agency’s decision raised red flags for opponents of the Affordable Care Act who argue the IRS violated the law. However, the government has said that in order for the law’s insurance reforms to be successful, nationwide subsidies are needed.
Now, the high court will decide whether the 36 states using HealthCare.gov are permitted to offer tax credits to their residents.
House Republicans Present Their Plan
The Supreme Court isn’t expected to announce a ruling on King v. Burwell until June. However, experts are looking to lawmakers on Capitol Hill to ready a transition plan should the court rule against the Obama administration.
If that happens, health policy experts estimate that approximately 5.5 million Americans could lose their subsidies and see the price of their premiums increase drastically, as the subsidies help keep the costs of health plans down.
“If the court rules against the administration, as any fair reading of the law would demand, millions of individuals and families will hit a major road block: They’ll be stuck with health insurance designed by Washington, D.C., they can’t afford,” Republicans Kline, Ryan and Upton wrote.
Kline, Ryan and Upton are chairman of the House Education and Workforce, Ways and Means, and Energy and Commerce Committees, respectively.
To mitigate the fallout from the increased cost in premiums and lost subsidies, the trio of lawmakers revealed their “off-ramp from Obamacare”—the result of a working group made of House Republicans that designed a proposal for those potentially affected by the Supreme Court’s decision.
The plan is made up of two parts: The first authorizes states to opt out of the Affordable Care Act’s coverage requirements and the employer and individual mandates. The second part of the plan would secure “advanceable” and “refundable” tax credits for states affected by the Supreme Court’s decision.
“So here’s the bottom line: Under Obamacare, government controls your choices,” the Republicans wrote. “Under our proposal, you will. You’ll get to pick a plan that works for you.”
Senate Counterparts Offer Their Ideas
Echoing the actions of their House counterparts, a trio of Republican Senate leaders penned their own op-ed in the Washington Post to discuss their answer to King v. Burwell.
Sens. Lamar Alexander, Orrin Hatch and John Barrasso, heads of the Senate Health, Education, Labor and Pensions Committee, Finance Committee and Republican Policy Committee, respectively, outlined their plan to help Americans at risk of losing their subsidies.
“When the court rules in King v. Burwell, we anticipate that it will hold the administration to the laws Congress passed, rather than the laws the administration wishes Congress had passed, and prohibit subsidies in states that opted not to set up their own exchanges, as the language of the law clearly states,” they wrote.
The senators’ plan includes providing financial assistance to affected Americans that would allow them to keep their original coverage for a “transitional period.”
“People do not deserve further disruption from this law,” they said.
Additionally, their plan would give power back to states and allow them to design their own health care system.
“[A ruling against the administration] would also give Congress an opportunity—to stop Obamacare’s damage and create a pathway to reforms that move our health care system in the direction of freedom, choice and lower cost,” Alexander, Hatch and Barrasso said.
Experts’ Ideas
The congressional Republicans are in lockstep with aspects of policy proposals offered by conservative experts in response to the Supreme Court’s decision.
Nina Owcharenko and Ed Haislmaier, health policy experts at The Heritage Foundation, outlined their answer to King v. Burwell in a paper released last week.
“Congress and the states should therefore seize the opportunity and clear the way for patient-centered, market-based reforms to take root in the states,” the pair wrote.
The experts encouraged Congress to exempt those in affected states from the Affordable Care Act’s insurance regulations, as well as the individual and employer mandates. Additionally, Owcharenko and Haislmaier advised lawmakers to pass pre-emptive legislation shifting plans from being federally regulated to state-regulated.
However, the experts advised Congress to abandon the “complex and costly subsidies of the ACA,” as they are accompanied by rules, restrictions and penalties.
“The design of the subsidies creates major financial incentive for millions of Americans to shift to plans that qualify for the new subsidies,” they wrote.
The Obama Administration’s Plan
White House officials contend that both those for and against the Affordable Care Act agreed that it was generally understood that those who joined the federal exchange were eligible for the law’s subsidies. And both the president and Health and Human Services Secretary Sylvia Mathews Burwell believe the Supreme Court will uphold the law as it’s currently interpreted.
However, neither the president nor Burwell said they have a contingency plan for if the high court rules the other way.
“We know of no administrative actions that could, and therefore we have no plans that would, undo the massive damage to our health care system that would be caused by an adverse decision,” Burwell wrote in a letter to Republicans last week.
In an interview with Reuters, the president echoed Burwell’s statements.
“If they rule against us, we’ll have to take a look at what our options are,” Obama said. “But I’m not going to anticipate that. I’m not going to anticipate bad law.”
>>> Commentary: What Alexander Hamilton Would Say About King v. Burwell
Content attributed to the Daily Signal








