HEALTH TRAIN EXPRESS
Mission: To promulgate health education across the internet:
Follow or subscribe to Health Train Express as well as Digital Health Space for all the updates for health policy, reform, public health issues. Health Train Express is published several times a week.Subscribe and receive an email alert each time it is published. Health Train Express has been published since 2006.
UnitedHealthcare, Cigna and Aetna move to revamp prior-authorization programs.
The paperwork required by health insurers to get many medical procedures or tests—one of the biggest gripes of doctors and patients—is getting rolled back.
UnitedHealth Group Inc.’s UnitedHealthcare, the largest health insurer in the U.S., said Wednesday it would cut its use of the prior authorization process. Starting in the third quarter, it will remove many procedures and medical devices from its list of services requiring signoff.
I go into a great deal about his issue in my Substack article Dreaded Medical Paperwork Required by Health Insurers to Be Trimmed
For more than two decades patients have heard their physician say I will have to obtain “prior authorization” from your insurance company for this test, drug, or treatment. The paperwork required by health insurers to get many medical procedures or tests—one of the biggest gripes of doctors and patients—is getting rolled back.
This is a major advance in eliminating physician ‘burnout’. Besides the use of electronic health records, many physicians have abandoned their dream of being doctors. Many have said this has become a moral dystopia for providers. For patients, it has meant delays in necessary treatments, causing anxiety, worsening health, and rarely death. It will eliminate stacks of paperwork, and endless waiting on hold to speak to an insurance representative.
Angus Worthing, a rheumatologist in Washington, D.C., whose practice has to employ roughly one prior-authorization-focused staffer for every two doctors, said. Patients typically wait two to four weeks to get medications under the process, he said, and while they wait, he sometimes needs to put them on other drugs that cause side effects. Several decades ago it was presumed that doctors ordered too many tests, and at times treatments that had no evidence for improvement of health. Prior authorizations were thought to decrease these occurrences. Initially, this had the immediate effect to reduce utilization.
You have probably forgotten that Obamacare (the Affordable Care Act) ensured that Health Insurance Companies cover preventive services. This includes immunizations, screening tests for cancer (mammograms, colon cancer, prostate cancer), blood pressure, diabetes, and cholesterol tests, physical exams and well-baby, well-child visits, HIV, and mental health services. Americans have benefited from this mandated coverage since 2010.
A Federal judge in Texas, who once said the ACA was unconstitutional, has struck down the requirement that preventive care be covered and that decision could affect more than 150 million people who would lose these "free" services. I say "free" because they are now covered under the exorbitant premiums that Insurance companies charge.
Insurers say that they will not claw back on this coverage that people have come to expect. But I see changes in formularies, co-pays, deductibles, and requirements for pre-authorization that seem to change month by month. I have absolutely no doubt that these preventive services will be whittled away one by one if this ruling is allowed to remain.
The ruling stemmed from a case brought by six individuals and two Christian-owned businesses who argued that they should not be mandated to offer coverage of HIV PrEP because they did not want to encourage "homosexual behavior."
Why make this change for these small businesses ? Do they want to "damn" those who have contracted HIV or prevent it? Has the Vatican taken a stand on this?
"Instead of attacking the coverage that patients have, we should be looking for ways to bolster the ACA and increase access to care." The US repeatedly ranks last in health outcomes compared to other industrialized nations and this will further widen the gap.
Today (Friday, March 31), President Biden appealed the decision and it will be heard in the US Fifth Circuit Court of Appeals. "All preventive services are kind of up for grabs as we go through the appeals process," said Laurie Sobel, associate director for women's health policy at Kaiser Family Foundation.
It may ultimately go to the US Supreme Court.
Let's see of the rule of law overturns common sense and the Affordable Care Act.
Malignancy may start small but always metastasizes
Two years after Abbott landed FDA clearance for a hand-held blood test that could detect signs of mild traumatic brain injuries (TBIs) in the span of about 15 minutes, the concussion-spotting test is heading to the big leagues.
The FDA has now cleared a version of the diagnostic that’s designed to run on Abbott’s Alinity i laboratory instruments. Because the Alinity systems are installed in hospitals and labs across the U.S., the regulatory clearance vastly scales up the availability of the test for the millions of Americans who experience concussions every year, Abbott noted in its Tuesday announcement. This vastly increases accessibility for clinicians from their office. The test is already available outside the U.S., having reeled in CE mark approval in Europe at the end of 2021.
The lab test works by analyzing a blood sample drawn from the arm. It looks for two biomarkers in the blood, both of which have been closely linked to TBIs when found in elevated concentrations. In studies, it was able to churn out results with 96.7% sensitivity and 99.4% negative predictive value, per Abbott.
The test returns results within about 18 minutes and has been authorized to assess patients aged 18 and older within 12 hours of a suspected concussion. It’s meant to be used as a triaging step before a CT scan, following a physician’s assessment of a patient’s visual, verbal and motor responses—which is often the only test they undergo before being sent off for a confirmatory CT scan.
According to Abbott, using the test as a first step in diagnosing concussion can help reduce the number of unnecessary CT scans performed on patients without actual brain injuries by as much as 40%—and will therefore cut down on the amount of time they need to spend in a hospital’s emergency department—while also flagging the patients who do need further imaging to confirm a concussion.
The newly FDA-cleared diagnostic offers a high-throughput alternative to Abbott’s i-STAT TBI Plasma test, which was given the green light to spot signs of traumatic brain injuries at the start of 2021.
That version of the concussion-detecting blood test runs on the i-STAT Alinity platform, a smartphone-sized, hand-held device that’s able to separate out plasma from a blood sample and conduct its biomarker analysis within 15 minutes.
A study published last year looked at the pair of biomarkers measured in both versions of the TBI test. After examining test results and longer-term outcome data for nearly 1,700 patients, the researchers concluded that higher concentrations of those biomarkers were linked to a higher probability of severe disability and death within six months of the initial brain injury.
SyncThink clocks FDA nod for concussion test based on AI-powered eye tracking
This device mimics the usual test of following a finger test given by an emergency room physician. Using AI it measures more accurately abnormal eye tracking movement and creates a graphic representation of the eye movement.
The Eye-Sync platform from SyncThink uses AI to analyze the results of a series of fast-paced eye-tracking assessments, in tandem with standard neurocognitive tests, patient records and reported symptoms, to determine the type and severity of cognitive dysfunction caused by a head injury.
The technology previously received 510(k) clearance from the FDA in 2016 for use in detecting impairments in patients’ gaze and visual tracking abilities. The new clearance extends the platform’s indications, allowing healthcare providers in the U.S. to use it to help diagnose both concussion and mild traumatic brain injury.
The Eye-Sync platform from SyncThink uses AI to analyze the results of a series of fast-paced eye-tracking assessments, in tandem with standard neurocognitive tests, patient records and reported symptoms, to determine the type and severity of cognitive dysfunction caused by a head injury.
The technology previously received 510(k) clearance from the FDA in 2016 for use in detecting impairments in patients’ gaze and visual tracking abilities. The new clearance extends the platform’s indications, allowing healthcare providers in the U.S. to use it to help diagnose both concussion and mild traumatic brain injury.
SyncThink isn’t the only medtech developer attempting to clear the thorny pathway to concussion diagnosis.
BrainScope, for one, added an FDA-cleared, concussion-detecting algorithm of its own to its point-of-care brain-scanning headset in March. The Concussion Index analyzes multiple EEG readings from the headset to monitor the progression of traumatic injuries, hidden bleeds and concussions.
Abbott, too, has thrown its hat in the ring. In January, the FDA doled out yet another clearance for concussion detection, this time for Abbott’s i-STAT Alinity platform, a hand-held rapid blood-testing system that measures the amount of certain proteins in the bloodstream after a head injury to determine whether further testing is required.
The Norfolk Southern train derailment in Ohio brought forth the real dangers of toxic chemical transportation via rail in the United States. The EPA and DOT have jurisdiction in these areas as guardians of public safety in transportation and environmental health.
These occurrences happen more than we like to know. Many trains may travel through your city or town with the local population being notified. Transportation routes are governed by the legal right of way granted when the lines are built.
In this particular case, vinyl chloride was being transported in large amounts for industrial purposes. Vinyl chloride, also called vinyl chloride monomer (VCM), is exclusively used as a precursor to PVC.(common use for producing pipes. Due to its hazardous nature, VCM is not found in other products. When burned vinyl chloride produces dioxin.
I emphasize the urgency of testing for dioxin exposure stemming from the East Palestine train catastrophe, and I publicly challenge the EPA, Gov. DeWine, and Sen. JD Vance to carry out dioxin testing across the affected areas. Dioxin residues are persistent, long term and reside in the soil. Senator Vance aptly displayed this 'dipstick test' which revealed the residue in a local creek, after the EPA declared the area as "safe" Safe for what?
According to some sources, the EPA has not done any dioxin testing at all. That's because they know they will find extreme levels of dioxins contaminating tens of thousands of acres of farmland, and Ohio exports over three billion dollars worth of agricultural products each year.
This event is not just local or regional, it has the potential to be a national emergency. Some of these agricultural products (animal and plant) are distributed nationally.
Capitalizing on the pandemic explosion in telehealth and therapy apps that collect details of your mental health needs, data brokers are packaging that information for resale, a new study finds. There’s no law stopping them.
One company advertised the names and home addresses of people with depression, anxiety, post-traumatic stress or bipolar disorder. Another sold a database featuring thousands of aggregated mental health records, starting at $275 per 1,000 “ailment contacts.”
Does your telehealth app sell your information? There is no law against it if they get your data.
HIPAA regulations protect your data in your electronic health records. However, there may be some telehealth applications that do not comply with HIPAA regulations.
The portions of HIPAA governing telemedicine are the Privacy Rule and the Security Rule. The HIPAA Privacy Rule sets standards to protect patient medical records or any personal health information (PHI) transmitted between health insurance companies, clinicians, testing facilities, or anywhere this data is shared.
If you are using an EHR portal or connect via a text link from your provider, the telehealth application is HIPAA compliant.
Decisions by CVS and Optum Panicked Thousands of Their Sickest Patients
Arthur Allen
NEW YORK — The fear started when a few patients saw their nurses and dietitians posting job searches on LinkedIn.
Word spread to Facebook groups, and patients started calling Coram CVS, a major U.S. supplier of the compounded IV nutrients on which they rely for survival. To their dismay, CVS Health confirmed the rumors on June 1: It was closing 36 of the 71 branches of its Coram home infusion business and laying off about 2,000 nurses, dietitians, pharmacists, and other employees.
Many of the patients left in the lurch have life-threatening digestive disorders that render them unable to eat or drink. They depend on parenteral nutrition, or PN — in which amino acids, sugars, fats, vitamins, and electrolytes are pumped, in most cases, through a specialized catheter directly into a large vein near the heart.
The day after CVS’ move, another big supplier, Optum Rx, announced its own consolidation. Suddenly, thousands would be without their highly complex, shortage-plagued, essential drugs and nutrients.
“With this kind of disruption, patients can’t get through on the phones. They panic,” said Cynthia Reddick, a senior nutritionist who was let go in the CVS restructuring.
“It was very difficult. Many emails, many phone calls, acting as a liaison between my doctor and the company,” said Elizabeth Fisher Smith, a 32-year-old public health instructor in New York City, whose Coram branch closed. A rare medical disorder has forced her to rely on PN for survival since 2017. “In the end, I got my supplies, but it added to my mental burden. And I’m someone who has worked in health care nearly my entire adult life.”
CVS had abandoned most of its less lucrative market in home parenteral nutrition, or HPN, and “acute care” drugs like IV antibiotics. Instead, it would focus on high-dollar, specialty intravenous medications like Remicade, which is used for arthritis and other autoimmune conditions.
Home and outpatient infusions are a growing business in the United States, as new drugs for chronic illness enable patients, health care providers, and insurers to bypass in-person treatment. Even the wellness industry is cashing in, with spa storefronts and home hydration services.
But while reimbursement for expensive new drugs has drawn the interest of big corporations and private equity, the industry is strained by a lack of nurses and pharmacists. And the less profitable parts of the business — as well as the vulnerable patients they serve — are at serious risk.
This includes the 30,000-plus Americans who rely for survival on parenteral nutrition, which has 72 ingredients. Among those patients are premature infants and post-surgery patients with digestive problems, and people with short or damaged bowels, often the result of genetic defects.
While some specialty infusion drugs are billed through pharmacy benefit managers that typically pay suppliers in a few weeks, medical plans that cover HPN, IV antibiotics, and some other infusion drugs can take 90 days to pay, said Dan Manchise, president of Mann Medical Consultants, a home care consulting company.
In the 2010s, CVS bought Coram, and Optum bought up smaller home infusion companies, both with the hope that consolidation and scale would offer more negotiating power with insurers and manufacturers, leading to a more stable market. But the level of patient care required was too high for them to make money, industry officials said.
“With the margins seen in the industry,” Manchise said, “if you’ve taken on expensive patients and you don’t get paid, you’re dead.”
In September, CVS announced its purchase of Signify Health, a high-tech company that sends out home health workers to evaluate billing rates for “high-priority” Medicare Advantage patients, according to an analyst’s report. In other words, as CVS shed one group of patients whose care yields low margins, it was spending $8 billion to seek more profitable ones.
CVS “pivots when necessary,” spokesperson Mike DeAngelis told KHN. “We decided to focus more resources on patients who receive infusion services for specialty medications” that “continue to see sustained growth.” Optum declined to discuss its move, but a spokesperson said the company was “steadfastly committed to serving the needs” of more than 2,000 HPN patients.
DeAngelis said CVS worked with its HPN patients to “seamlessly transition their care” to new companies.
However, several Coram patients interviewed about the transition indicated it was hardly smooth. Other HPN businesses were strained by the new demand for services, and frightening disruptions occurred.
Smith had to convince her new supplier that she still needed two IV pumps — one for HPN, the other for hydration. Without two, she’d rely partly on “gravity” infusion, in which the IV bag hangs from a pole that must move with the patient, making it impossible for her to keep her job.
“They just blatantly told her they weren’t giving her a pump because it was more expensive, she didn’t need it, and that’s why Coram went out of business,” Smith said.
Many patients who were hospitalized at the time of the switch — several inpatients stays a year are not unusual for HPN patients — had to remain in the hospital until they could find new suppliers. Such hospitalizations typically cost at least $3,000 a day.
“The biggest problem was getting people out of the hospital until other companies had ramped up,” said Dr. David Seres, a professor of medicine at the Institute of Human Nutrition at Columbia University Medical Center. Even over a few days, he said, “there was a lot of emotional hardship and fear over losing long-term relationships.”
To address HPN patients’ nutritional needs, a team of physicians, nurses, and dietitians must work with their supplier, Seres said. The companies conduct weekly bloodwork and adjust the contents of the HPN bags, all under sterile conditions because these patients are at risk of blood infections, which can be grave.
As for Coram, “it’s pretty obvious they had to trim down business that was not making money,” Reddick said, adding that it was noteworthy both Coram and Optum Rx “pivoted the same way to focus on higher-dollar, higher-reimbursement, high-margin populations.”
“I get it, from the business perspective,” Smith said. “At the same time, they left a lot of patients in a not great situation.”
***
Smith shares a postage-stamp Queens apartment with her husband, Matt; his enormous flight simulator (he’s an amateur pilot); cabinets and fridges full of medical supplies; and two large, friendly dogs, Caspian and Gretl. On a recent morning, she went about her routine: detaching the bag of milky IV fluid that had pumped all night through a central line implanted in her chest, flushing the line with saline, injecting medications into another saline bag, and then hooking it through a paperback-sized pump into her central line.
Smith has a connective tissue disorder called Ehlers-Danlos syndrome, which can cause many health problems. As a child, Smith had frequent issues such as a torn Achilles tendon and shoulder dislocations. In her 20s, while working as an EMT, she developed severe gut blockages and became progressively less able to digest food. In 2017, she went on HPN and takes nothing by mouth except for an occasional sip of liquid or bite of soft food, in hopes of preventing the total atrophy of her intestines. HPN enabled her to commute to George Washington University in Washington, D.C., where in 2020 she completed a master’s in public health.
On days when she teaches at LaGuardia Community College — she had 35 students this semester — Smith is up at 6 a.m. to tend to her medical care, leaves the house at 9:15 for class, comes home in the afternoon for a bag of IV hydration, then returns for a late afternoon or evening class. In the evening she gets more hydration, then hooks up the HPN bag for the night. On rare occasions she skips the HPN, “but then I regret it,” she said. The next day she’ll have headaches and feel dizzy, sometimes losing her train of thought in class.
Smith describes a “love-hate relationship” with HPN. She hates being dependent on it, the sour smell of the stuff when it spills, and the mountains of unrecyclable garbage from the 120 pounds of supplies couriered to her apartment weekly. She worries about blood clots and infections. She finds the smell of food disconcerting; Matt tries not to cook when she’s home. Other HPN patients speak of sudden cravings for pasta or Frosted Mini-Wheats.
Yet HPN “has given me my life back,” Smith said.
She is a zealous self-caretaker, but some dangers are beyond her control. IV feeding over time is associated with liver damage. The assemblage of HPN bags by compounding pharmacists is risky. If the ingredients aren’t mixed in the right order, they can crystallize and kill a patient, said Seres, Smith’s doctor.
He and other doctors would like to transition patients to food, but this isn’t always possible. Some eventually seek drastic treatments such as bowel lengthening or even transplants of the entire digestive tract.
“When they run out of options, they could die,” said Dr. Ryan Hurt, a Mayo Clinic physician and president of the American Society for Parenteral and Enteral Nutrition.
***
And then there are the shortages.
In 2017, Hurricane Maria crippled dozens of labs and factories making IV components in Puerto Rico; next came the covid-19 emergency, which shifted vital supplies to gravely ill hospital patients.
Prices for vital HPN ingredients can fluctuate unpredictably as companies making them come and go. For example, in recent years the cost of the sodium acetate used as an electrolyte in a bag of HPN ballooned from $2 to $25, then briefly to $300, said Michael Rigas, a co-founder of the home infusion pharmacy KabaFusion.
“There may be 50 different companies involved in producing everything in an HPN bag,” Rigas said. “They’re all doing their own thing — expanding, contracting, looking for ways to make money.” This leaves patients struggling to deal with various shortages from saline and IV bags to special tubing and vitamins.
“In the last five years I’ve seen more things out of stock or on shortage than the previous 35 years combined,” said Rigas.
The sudden retrenchment of CVS and Optum Rx made things worse. Another, infuriating source of worry: the steady rise of IV spas and concierge services, staffed by moonlighting or burned-out hospital nurses, offering IV vitamins and hydration to well-off people who enjoy the rush of infusions to relieve symptoms of a cold, morning sickness, a hangover, or just a case of the blahs.
In January, infusion professionals urged FDA Commissioner Robert Califf to examine spa and concierge services’ use of IV products as an “emerging contributing factor” to shortages.
Bracha Banayan’s concierge service, called IVDRIPS, started in 2017 in New York City and now employs 90 people, including 60 registered nurses, in four states, she said. They visit about 5,000 patrons each year, providing IV hydration and vitamins in sessions of an hour or two for up to $600 a visit. The goal is “to hydrate and be healthy” with a “boost that makes us feel better,” Banayan said.
Although experts don’t recommend IV hydration outside of medical settings, the market has exploded, Banayan said: “Every med spa is like, ‘We want to bring in IV services.’ Every single paramedic I know is opening an IV center.”
Matt Smith, Elizabeth’s husband, isn’t surprised. Educated as a lawyer, he is a paramedic who trains others at Columbia University Irving Medical Center. “You give someone a choice of go up to some rich person’s apartment and start an IV on them, or carry a 500-pound person living in squalor down from their apartment,” he said. “There’s one that’s going to be very hard on your body and one very easy on your body.”
The very existence of IV spa companies can feel like an insult.
“These people are using resources that are literally a matter of life or death to us,” Elizabeth Smith said.
For five months last year, Rylee Cornwell, 18 and living in Spokane, Washington, could rarely procure lipids for her HPN treatment. She grew dizzy or fainted when she tried to stand, so she mostly slept. Eventually she moved to Phoenix, where the Mayo Clinic has many Ehlers-Danlos patients and supplies are easier to access.
Mike Sherels was a University of Minnesota Gophers football coach when an allergic reaction caused him to lose most of his intestines. At times he’s had to rely on an ethanol solution that damages the ports on his central line, a potentially deadly problem “since you can only have so many central access sites put into your body during your life,” he said.
When Faith Johnson, a 22-year-old Las Vegas student, was unable to get IV multivitamins, she tried crushing vitamin pills and swallowing the powder, but couldn’t keep the substance down and became malnourished. She has been hospitalized five times this past year.
Dread stalks Matt Smith, who daily fears that Elizabeth will call to say she has a headache, which could mean a minor allergic or viral issue — or a bloodstream infection that will land her in the hospital.
Even more worrying, he said: “What happens if all these companies stop doing it? What is the alternative? I don’t know what the economics of HPN are. All I know is the stuff either comes or it doesn’t.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
I have decided to take a respite from blogging. I see my readership has declined due to changes in the algorithm, and other changes in the internet space, such as Metaverse, Web3, AR, VR, and AI.
Cochrane Library has existed for 35 years. I was a young physician when it came into existence. Its publication was based on real clinical results. I its infancy few physicians even knew about it rarely referring to it for treatment recommendations. The gold standard was the New England Journal of Medicine and the National Library of Medicine, or specialty journals and reviews.
Now it ranks up there with those bastions of information. Cochrane is for anyone interested in using high-quality information to make health decisions. Whether you are a clinician, patient or carer, researcher, or policy-maker, Cochrane evidence provides a powerful tool to enhance your healthcare knowledge and decision-making.
Cochrane's members and supporters come from more than 190 countries, worldwide. We are researchers, health professionals, patients, carers, and people passionate about improving health outcomes for everyone, everywhere. Our global independent network gathers and summarizes the best evidence from research to help you make informed choices about treatment and we have been doing this for 30 years.
We do not accept commercial or conflicted funding. This is vital for us to generate authoritative and reliable information, working freely, unconstrained by commercial and financial interests.
Unfortunately, Cochrane is rarely quoted or referred to as a source of reliable information by the national media, social media, or even google. It does not appear on page one in my google searches for medical information, or treatment plans. Cochrane has become sensitized to this lack of visibility and initiated an RCT (Randomized Clinical Trial)) to evaluate what the impact of using Twitter to disseminate Cochrane Reviews as a source of information.
I want to highlight what just came out: the Cochrane review on masking. It shows that community mask recommendations have no firm data to support them. The authors write:
“There is a need for large, well-designed RCTs addressing the effectiveness of many of these interventions in multiple settings and populations, as well as the impact of adherence on effectiveness, especially in those most at risk”
Let me be clear: The science did not change. Public health experts started lying. We never had good data that mask mandates help, or that mask advice (a softer policy) improves outcomes. Yet it was widely pushed— most likely to distract from true federal failures.
After vaccination, not only do we not have evidence. It is irrational to mask. At best you marginally delay the inevitable, and unlike pre-vax, there is no milestone you are waiting for. Let’s take a closer look.
Here is the big summary finding. With 276,000 participants in RCTs or cluster RCTs, masking does nothing. No reduction in influenza-like or Covid like illness and no reduction in confirmed flu or COVID. That’s stone-cold negative. See those effect sizes and confidence intervals.
Masks have no good data to support them| It is a religion, not a science.
Three years later most of the SARS-Covid viral epidemic has dissipated but still remains endemic. In other words, it is with us 'forever'. Covid is now relegated to the ordinary flu-like syndrome. The risk of long Covid remains as a small percentage of overall Covid infection. Now we have a risk of adverse reactions to Covid vaccination.
Covid vaccination gave birth to msRNA production of a portion of the virus capsid, in this case, a protein spike. The newer form produces a myriad of complications that are not seen in the classical vaccines produced by attenuated whole vaccines. Covid 19 mutated rapidly through a number of mutations too numerous to elaborate in this article.
As Covid has evolved, so too have vaccinations and treatments. In the world of virology, small things matter (no pun intended) and small things rapidly evolve.
61% of circulating variants are now XBB.1.5 and 22% BQ.1.1 – what use are C19 mRNA injections targeting BA.4 and BA.5?
“As of January 20, 2023, >90% of circulating SARS-CoV-2 variants in the United States, specifically Omicron BQ.1, BQ.1.1, XBB, and XBB.1.5 sublineages, are unlikely to be susceptible to the combined monoclonal antibodies, tixagevimab and cilgavimab (Evusheld) used for preexposure prophylaxis against SARS-CoV-2 infection (1).
“The FDA pulled Evusheld because it is not effective against 95% of the omicron subvariants circulating in the U.S. This includes the XBB subvariants which are now causing 64% of new cases, as well as the BQ family that is responsible for 31% of reported infections.”
The latest variants estimated to be circulating in the US from the CDC
With a tabulation of the current estimated prevalence of each variant here:
The Food and Drug Administration announced on January 26, 2023, that Evusheld is not currently authorized for preexposure prophylaxis against SARS-CoV-2 infection in the United States (2). It is important that persons who are moderate to severely immunocompromised,* those who might have an inadequate immune response to COVID-19 vaccination, and those with contraindications to receipt of COVID-19 vaccines, exercise caution and recognize the need for additional preventive measures (Box). In addition, persons should have a care plan that includes prompt testing at the onset of COVID-19 symptoms and rapid access to antivirals if SARS-CoV-2 infection is detected
For those with an immunocompromised system here is a plan:
Personal COVID-19 action plan§ (only for those with compromised immune systems) Not for the general public.
Persons should consider how to protect themselves and others around them should they become ill with COVID-19 or if the community's COVID-19 transmission level changes. The plan should include:
ways to protect oneself and others including considerations in case of illness, such as finding a room in which to isolate actions to take in case of exposure or symptom onset, what to do in the event of receipt of a positive SARS-CoV-2 test result
Persons should share their COVID-19 plan with their families, friends, and healthcare providers so they can support prevention and preparation steps. CDC suggests that people consider how others can help them if they get ill. It is important to adhere to treatment plans, keep routine healthcare appointments, and ensure that prescriptions are filled. Persons should make alternative plans for work, child care, and other responsibilities that might cause stress if they become ill.
One-third of Americans die of Alzheimer's Disease (AD). During the past decade, early diagnosis has improved but can be problematic. A standard medical workup for Alzheimer's disease often includes structural imaging with magnetic resonance imaging (MRI) or computed tomography (CT). These tests are primarily used to rule out other conditions that may cause symptoms similar to Alzheimer's but require different treatments. There are no specific blood tests, nor imaging test that is diagnostic for AD
How is AD diagnosed? AD is often a rule-out illness, by eliminating other causes of dementia.
What causes dementia?
Common causes of dementia are:
Alzheimer's disease. This is the most common cause of dementia.
Vascular dementia. This may occur in people who have long-term high blood pressure, severe hardening of the arteries, or several small strokes. Strokes are the second most common cause of dementia.
Parkinson's disease. Dementia is common in people with this condition.
Dementia with Lewy bodies. It can cause short-term memory loss.
Frontotemporal dementia. This is a group of diseases that includes Pick's disease.
Severe head injury.
Less common causes of dementia include:
Huntington's disease.
Leukoencephalopathies. These are diseases that affect the deeper, white-matter brain tissue.
Creutzfeldt-Jakob disease. This is a rare and fatal condition that destroys brain tissue.
Some cases of multiple sclerosis (MS) or amyotrophic lateral sclerosis (ALS).
Multiple-system atrophy. This is a group of degenerative brain diseases that affect speech, movement, and autonomic function.
Infections such as late-stage syphilis. Antibiotics work well to treat syphilis at any stage, but they can't reverse the brain damage already done.
Inherited dementia
Some disorders that cause dementia can run in families. Doctors often suspect an inherited cause if someone younger than 50 has symptoms of dementia.
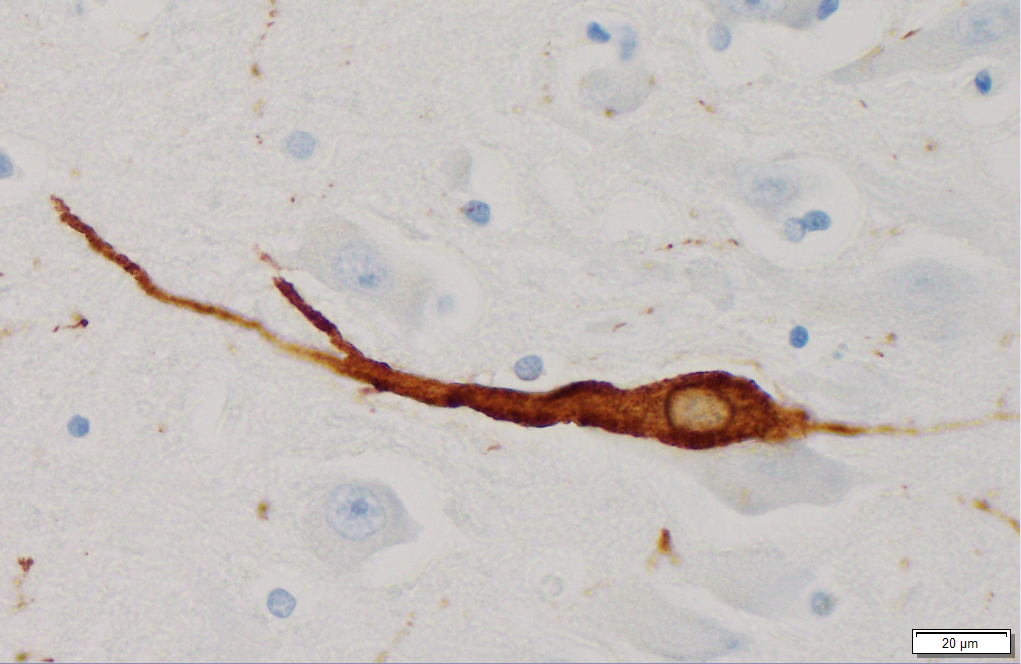
The classical pathologic signs are the neurofibrillary tangle and the senile plaque. The neurofibrillary tangle consists of abnormal accumulations of abnormally phosphorylated tau within the perikaryal cytoplasm of certain neurons. Tau is an abnormal protein that accumulates within the neurons.
Microtubules in neurons
Amyloid plaques are aggregates of misfolded proteins that form in the spaces between nerve cells. These abnormally configured proteins are thought to play a central role in Alzheimer's disease. The amyloid plaques first develop in the areas of the brain concerned with memory and other cognitive functions. Amyloid plaques form one of the two defining features of Alzheimer’s disease, the other being neurofibrillary tangles.
Amyloid Plaques
Neurofibrillary tau
The impact of AD is enormous in terms of caregiving, and support services. Many families cannot afford the full-time support necessary for a parent or loved one. Assisted living and/or memory support units are expensive, and most health insurance does not reimburse for those services.
Unlike heart disease where progress has been significant in diagnosis and treatment, AD presents other challenges, such as being difficult to diagnose and a lack of proven treatments.
Can Alzheimer's Disease Be Prevented? We know that control of blood pressure, lowering blood lipids, and regular exercise can reduce the risk of atherosclerotic heart disease.
Which came first? The chicken or the egg? Are the tangles and amyloid the result of dementia, or do tangles and amyloid cause dementia?
Financial repercussions for the health system (Medicare/Medicaid)
In 2015, the costs to all payers for the care of people living with Alzheimer's disease and other dementias will total an estimated $226 billion, with Medicare and Medicaid paying 68 percent of the costs. Without a treatment, costs are projected to increase to more than $1.1 trillion in 2050.
A treatment introduced in 2025 that delays the onset of Alzheimer's would cut the number of people in 2050 who have the disease by 42 percent — from 13.5 million to 7.8 million. The Alzheimer's Association's report also shows the positive impact of adequate funding and the potential consequences of underfunding.
Reaching the 2025 goal would save payers $220 billion over the first five years and $367 billion in 2050 alone. Savings to Medicare and Medicaid would account for nearly 60 percent of the savings.
Notwithstanding the financial advantages, there is another and perhaps more important item, quality of life
Short of finding a successful treatment, advanced directives are proactive and allow for seniors to instruct their surviving children and relatives as to what you want. The Advanced Directive must be filed with your physician and/or hospital.
In its year-end omnibus legislation passed on December 23, 2022, Congress took steps to a expand access to medication-assisted treatment for opioid use disorder. Under the new law, physicians no longer must obtain a special federal waiver to prescribe buprenorphine, which is used to treat patients with opioid use disorder.
The California Medical Association (CMA) supports efforts to increase access to much-needed medication-assisted treatment for opioid use disorders. Across the country, many people suffering from opioid use disorder are unable to access medication-assisted treatment for their condition due to a lack of nearby physicians with waivers to prescribe buprenorphine.
Going forward, all prescriptions for buprenorphine only require a standard U.S. Drug Enforcement Agency (DEA) registration number. Additionally, there are no longer any limits or patient caps on the number of patients a prescriber may treat for opioid use disorder with buprenorphine.
Section 1263 of the Omnibus spending bill (the Medication Access Training Expansion Act) also establishes new training requirements for all prescribers of controlled substances, which will take effect June 21, 2023. The new law requires all prescribers of schedule II – V controlled substances to meet a one-time eight-hour training requirement on identifying, treating, and managing patients with opioid or other substance use disorders. (Certain physicians – including those board certified in addiction medicine – will be deemed to have met this training requirement through their specialty training and/or board certification. Click here for more details.)
Congress eliminates need for waiver to treat opioid use disorder: In its year-end omnibus legislation, Congress took steps to a expand access to medication-assisted treatment for opioid use disorder. Under the new law, physicians no longer must obtain a special fed...